
Facial cosmetic surgery focuses on improving the appearance of the face. Common cosmetic surgery procedures include rhinoplasty, blepharoplasty (eyelid surgery), facelift, brow lift, chin augmentation, otoplasty (ear repositioning), liposuction, and fat transfer. Many patients may seek surgical treatment to reverse changes that occur with ageing, such as loose skin, decreased volume around the face and neck, crow’s feet at the outer part of the eyes, fine lines on the forehead, loss of jawline contour, sagging jowls, and a double chin.
Rhinoplasty
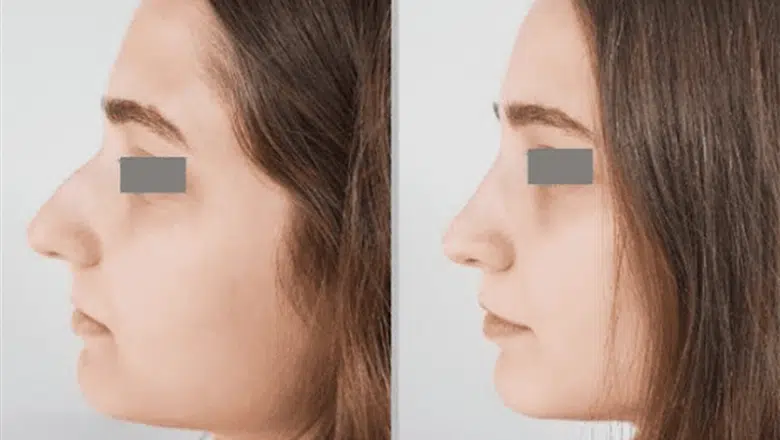
Perhaps the most commonly performed and most difficult facial plastic surgery is rhinoplasty. It is performed to correct intrinsic and extrinsic nasal pathology, modify the unsatisfactory aesthetic appearance, reduce airway obstruction (due to septal deviation, inferior turbinate hypertrophy or deviated/fractured nasal bones), and reconstruct congenital nasal anomalies present from birth. During a rhinoplasty, the nasal skin, subcutaneous soft tissue, cartilaginous and bony framework, and mucous membrane lining are manipulated surgically. The open rhinoplasty is differentiated from the closed or endonasal rhinoplasty in that the incision is made in the columella (fleshy tip of the nose that separates the nostrils) in the open approach. The general principle of rhinoplasty consists of separating the nasal skin and soft tissues from the bony and cartilaginous nasal framework so that the underlying nasal framework can be reshaped to produce the desired nasal contours. Rhinoplasty is a technically challenging procedure with 4 to 20% complication rates. Postoperative scarring and swelling, as well as patient dissatisfaction, can lead to revision rhinoplasty (secondary rhinoplasty).
RELATED: All about Rhinoplasty
Over the past ten years, rhinoplasty surgery has trended toward using structural techniques requiring cartilage tissue to reconstruct shape, reinforce weak parts of the nose, expand the airway, and create an aesthetic contour instead of destructive cartilage removal techniques. Advances in this area include the broader use of cartilage for structural grafting. Traditionally, rib cartilage was used for only major reconstructive nasal operations, but more recently, the number and type of grafts used in rhinoplasty have increased significantly as rib graft use became more prevalent in even primary cosmetic rhinoplasty. Digital imaging has become an increasingly important element of rhinoplasty planning, essential to preoperative consultations. Most surgeons now widely use three-dimensional (3-D) imaging systems and 3-D image morphing technologies, though no universally accepted software platform exists.
Blepharoplasty

Another popular facial procedure is blepharoplasty or eyelid surgery. Blepharoplasty involves the excision of excessive eyelid skin and/or removal of prolapsed fat to treat ageing-related changes in the eye region and reduce excessive wafer-thin skin. The impact of gravity on peri-ocular features reduced strength in periorbital muscles as a result of soft tissue laxity, chronic sun damage, and changes in the skin thickness may cause aesthetically unappealing changes referred to as “droopy eyelids”, “tired eyes”, or “bags under the eyes.” The usual technique for lower blepharoplasty surgery is through a lower eyelid incision with a raised skin and muscle flap, followed by identification and correction of prolapsed areas of fat.
The “skin pinch” blepharoplasty is the easiest to perform. This technique removes excess skin through the same approach as a traditional lower blepharoplasty. This method avoids a heavy skin–muscle flap, which can create potential pulling on the lower eyelid, leading to an ectropion. The pinch blepharoplasty of the lower lid also avoids violation of the orbicularis oculi muscle and the orbital septum to avoid nerve injury and decrease scarring. This approach allows more wrinkled, thin skin to be safely removed and an aesthetic eyelid position to be maintained. Both upper and lower-lid blepharoplasties are often performed under local anaesthesia with or without sedation. Of note is that blepharoplasty is also performed to correct eyelid sagging, which can arise from several causes. The most common cause is the weakness of the levator muscle.
Brow lift
Brow lift or browpexy is a large part of a facial plastic surgery practice.
RELATED: What is a Brow Lift?
This procedure is relatively straightforward in terms of its classical approach, where excess skin is resected, and the forehead skin is repositioned to a higher level. If the hairline is low, the incisions are placed along a line within the hair-bearing scalp. A hairline incision is used in patients with a high hairline. These two approaches are most commonly used in women. In men, a third option is a mid-brow lift, where an incision is made in a deep brow furrow on the forehead, and an ellipse of skin is removed. A direct brow lift is rarely performed, where the incision is made at the upper margin of the eyebrows. Both mid- and direct brow lifts may leave a visible scar, and they are more commonly used for functional brow surgery in patients who have significant brow drooping contributing to a disturbance of vision.
RELATED: Benefits of Brow Lift Surgery
The newest approach is the endoscopic brow lift, where several small incisions are placed behind the hairline, and an endoscope is used for visualisation during the elevation of the forehead skin. With the endoscope under the forehead flap, the surgeon releases soft tissue from the lower brow, allowing repositioning and fixation of the skin to be higher. The results are less dramatic, but it is an excellent technique for younger patients who prefer more natural and less defined changes.
Facelift

The facelift, known as rhytidectomy, is a commonly performed surgical facial rejuvenation procedure by expert facial plastic surgeons. When facelifts were first developed over 100 years ago, the procedure involved making multiple incisions and pulling the skin on the face tighter. The traditional incision is made in front of the ear, extending up into the hairline and curving around the bottom of the ear lobe and then behind the ear. The skin is separated from the deeper tissues, and then the deeper tissues are tightened with stitches. In the final step, the skin is repositioned with the excess skin removed.
The demands and desires of patients have largely driven advancements in facelift procedures. Patients today are looking for minimally invasive procedures with little to no postoperative downtime. Treatment of the ageing face has been profoundly impacted by the rise of so-called “lunchtime facelift” procedures. In the mid-1990s, facelifts and rejuvenation operations were becoming increasingly technically demanding and risky due to exposure of the facial nerve branches and extensive soft tissue dissections. These complex procedures gave Great results in expert hands.
RELATED: Does a Weekend Face Lift Really Work?
However, often, patients operated on by more junior surgeons experienced prolonged postoperative swelling, potential facial nerve injury, and facial asymmetry. Today, there are many facelift approaches, such as the deep plane facelift, composite facelift (which involves repositioning and fixation of the orbicularis oculi muscle), mid-facelift, mini-facelift, thread lift, skin-only facelift, and minimal access cranial suspension lift or MACS lift. Each can achieve outstanding outcomes but largely depends upon surgical skill and the anatomical variations between patients. In the early part of the 21st century, there was a rise in less invasive procedures, which could be performed under local anaesthesia with oral sedation. Overall, the number of facelifts has increased because of the marketing of the large UK cosmetic surgery chains. According to the British Society of Plastic Surgeons, facelifts have increased. A major trend in recent years is the combination of facelift operations with facial fat grafting or autologous fat transfer, which also addresses the volume loss that occurs with the ageing face.
Otoplasty

Otoplasty, also known as pinnaplasty or ear reshaping, is the surgical procedure to treat congenitally prominent ears. Otoplasty can be either cartilage splitting or cartilage preserving. Cartilage-splitting techniques involve incisions through the cartilage and repositioning of large portions of ear cartilage. Cartilage-sparing techniques avoid full-thickness incisions but create angles and curls in the cartilage for contouring. Most surgeons now perform cartilage-sparing otoplasty routinely.
Interested in a Facial Cosmetic Procedure? Contact Centre for Surgery Today
Are you considering a facial cosmetic procedure to enhance your appearance? Centre for Surgery offers a range of advanced treatments to help you achieve your aesthetic goals. Our team of highly skilled surgeons is committed to providing personalised care and outstanding results.
Whether you are looking to rejuvenate your skin, refine facial contours, or address specific concerns, we have the expertise to help you look and feel your best. Our comprehensive services include facelifts, rhinoplasty, blepharoplasty, lip lifts, and more.
Contact Centre for Surgery today to book a consultation. Our friendly and knowledgeable team will be happy to discuss your options, answer any questions you may have, and guide you through the process to ensure you make an informed decision.
Take the first step towards enhancing your natural beauty. Reach out to us and schedule your consultation now. We look forward to helping you achieve your desired results.






